SSRI
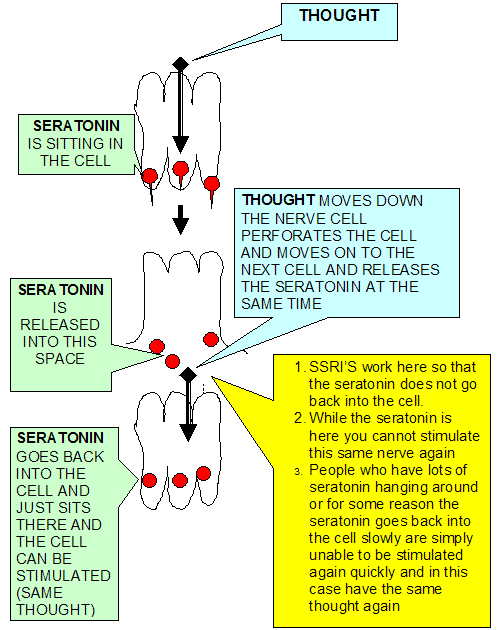
Major depression in response to stressful situations has been reported as more common among persons harboring a variant in the proximal 5' regulatory region of the gene encoding the serotonin-transporter protein (5-HTT) (the target of selective serotonin-reuptake inhibitors [SSRIs]) that modifies promoter activity. This variant, in the 5-HTT genelinked promoter region (5-HTTLPR), modifies promoter activity and is associated with lower transcriptional efficiency of the 5-HTT gene, ultimately leading to fewer copies of the messenger RNA encoding the serotonin-transporter protein.23 This lower-expressing variant may be associated with the amygdala-mediated hyperresponsiveness of young children to frightened or frightening faces that can facilitate encoding of painful memories, leading to stress sensitivity in adulthood.24 This variant is also associated with a reduction of serotonin function in response to maternal deprivation in nonhuman primates, an effect that persists into adulthood.25 An induced functional deficiency of the 5-HTT protein that is confined to the early postnatal period in mice results in altered behavior when they are grown, indicating possible changes in brain development that affect adult behavior.26
.
COMPARATIVE WEIGHT CHANGES BETWEEN SSRIs
J Clin Psychiatry. 2004;65:1365-1371
Among SSRIs, paroxetine is associated with weight gain early in therapy but the long-term effects are undear. Fluoxetine may cause short-term weight loss that resolves with continued treatment. Other SSRIs are either weight-neutral or the effects have yet to be determined. Nefazodone appears less likely to cause weight gain dun SSRIs. Bupropion is often associated with weight loss while mirtazapine is associated with weight gain and the effects of venlafaxine remain unclear
The largest trial prospectively comparing the metabolic effects of SSRIs was conducted by Maina et al.5 Patients with obsessive-compulsive disorder were randomized to treatment with clomipramine, citalopram, fluoxetine, fluvoxamine, paroxetine or sertraline for 2.5 years. Over the course of the trial, mean body weight increased by 1.58 kg (2.5%) compared to baseline, with 14.5% of patients experiencing significant weight gain (increase of 7% or more from baseline). Patients in the clomipramine group experienced the highest mean percentage weight increase (4.86%) and the highest proportion of significant weight gain (34.8%); this is consistent with the known adverse effects of TCAs. Fluoxetine patients experienced initial weight loss, and were the only treatment group to not experience significant weight gain over the course of the trial. The lowest proportions of patients experiencing significant weight gain were 8.7% and 4.5%, in the fluoxetine and sertraline groups, respectively. Trial results are summarized in the table below.
In another prospective trial evaluating long-term weight change, depressed patients were randomized to fluoxetine, sertraline, or paroxetine for 26 to 32 weeks.6 There was a small mean decrease in weight (0.2%) among fluoxetine patients and a small mean increase in weight (1.0%) among sertraline patients; neither change was statistically significant. Paroxetine-treated patients experienced a significant increase in weight compared with baseline (3.6%). From baseline to endpoint, 25.5%, 6.8% and 42% of paroxetine, fluoxetine and sertraline patients, respectively, experienced 7% or greater weight gain (P = 0.016 paroxetine vs fluoxetine, P = 0.003 paroxetine vs sertraline).
When fluoxetine was compared to placebo for the prevention of relapse after acute treatment of depression, fluoxetine was associated with significantly more weight gain than placebo over one year.7 After twelve weeks of acute treatment, fluoxetine was associated with slight weight loss (mean -0.35 kg, P
Newer, non-SSRI antidepressants have variable effects on weight. A pooled analysis of trials comparing nefazodone to SSRIs demonstrated that nefazodone is associated with fewer instances of significant (⥠7%) weight loss in the acute phase (6-8 weeks) of treatment.8 During the long-term treatment phase (16-44 weeks), fewer nefazodone than SSRI patients experienced significant (⥠7%) weight gain (8.3% vs. 17.9%, P = 0.003 for any point during treatment and 6.9% vs. 13.8%, P = 0.007 at endpoint). There was no difference between groups in the incidence of significant weight loss (⥠7%) during long-term treatment. Fewer instances of weight loss during the acute phase and weight gain during long-term therapy suggest that nefazodone causes less weight variability than SSRIs.
The weight gain associated with mirtazapine may be due to its activity at histamine receptors.9 In a long-term continuation of a trial of acute treatment, patients continued treatment with mirtazapine, amitriptyline, or placebo for up to two years.10 Weight gain was more common with amitriptyline (22%) than mirtazapine (13%) patients, but significantly more mirtazapine than placebo patients experienced weight gain. In a four-week study of healthy subjects, those treated with mirtazapine experienced a significant increase in body weight from baseline (mean increase 3.64 lb.), suggesting that the weight gain caused by mirtazapine is independent of the weight changes associated with recovering depression.11 This trial also quantified the changes in total cholesterol, LDL and triglycerides associated with mirtazapine treatment.11 After four weeks of therapy, mirtazapine-treated subjects experienced a significant increase in total cholesterol (mean increase 7.6 mg/dL) and nonsignificant increases in LDL and triglyceride levels compared to baseline, while no significant changes were noted in placebo-treated patients. Among treated patients, weight increase was linearly associated with increasing total cholesterol. The results of this short-term trial suggest that weight and cholesterol changes associated with mirtazapine occur independent of depression recovery.
A small, open-label trial compared the effects of mirtazapine and venlafaxine on weight.12 During the four weeks of treatment, mirtazapine-treated patients experienced a mean weight gain of 2.4 kg while venlafaxine-treated patients had a mean loss of 0.4 kg. A twelve-week trial did not detect weight change with either venlafaxine- or fluoxerine-treated patients.13 In another trial, weight changes in elderly patients treated with venlafaxine or citalopram for six months were not clinically significant.14 More research is needed to clarify the effects of venlafaxine on weight, although the agent is most likely not associated with significant weight gain or loss.
Bupropion is generally associated with weight loss. In an eight-week trial comparing sustained release (SR) bupropion 150-400 mg/day to sertraline 50-200 mg/day, bupropion patients experienced a mean 1.06 kg decrease in weight from baseline to endpoint compared with 0.79 kg decrease for sertraline and a 0.21 kg increase for placebo; these differences were not statistically significant.15 During an eight-week placebo-controlled trial, bupropion SR 300 mg/day and 400 mg/day caused weight loss greater than 5 pounds in 14% and 19% of patients, respectively, compared with 6% of placebo patients. Weight loss of greater than 10 pounds occurred in 2%, 6% and 2% of bupropion 300 mg, 400 mg and placebo patients.2